
- persistent atrial fibrillation,
- peAF,
- fibrotic atrial myopathy,
- ablation
Introduction | Objectives: Ablation of persistent atrial fibrillation (peAF) is associated with a worse outcome. Fibrotic atrial myopathy (FAM) is thought to play a role in the progression of AF. Estimation of left atrial voltage can vary significantly based on whether mapping is performed in fibrillatory conduction or sinus rhythm (SR). Selection of a voltage scale (VS) may lead to an over/under estimation of FAM. We determined the prevalence of advanced atrial myopathy (FAM > = 2) in SR compared to historical cohort ablated in peAF.
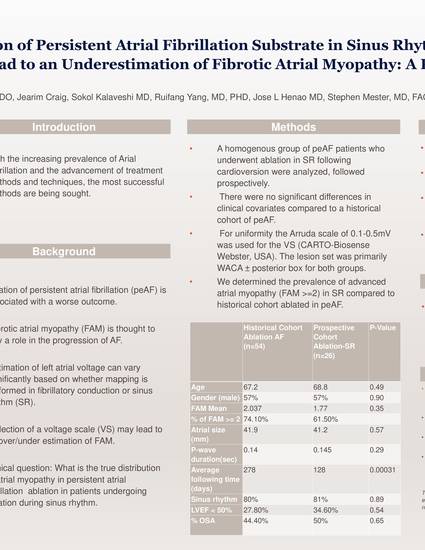
Methods: A homogenous group of peAF patients who underwent ablation in SR following cardioversion were analyzed, followed prospectively. There were no significant differences in clinical covariates compared to a historical cohort of peAF. For uniformity the Arruda scale of 0.1‐0.5 mV was used for the VS (CARTO‐Biosense Webster, USA). The lesion set was primarily WACA ± posterior box for both groups
Results: 26 patients were followed prospectively and compared to 54 historical peAF patients. There was no statistical difference in the major clinical variables between both groups (Figure 1). The historical cohort 74% [95% CI, 60 to 85] had FAM > = 2, while the SR group exhibited 62% [95% CI, 41 to 80]. There was no difference in clinical outcome achieving SR with 80% and 81% for the historical and study groups (P = 0.89).
Conclusions: Preliminary data would suggest that mapping either in AF or SR is acceptable for determining the extent of FAM in this population to guide a substrate‐based ablation strategy.
Abstract published in the Journal of Cardiovascular Electrophysiology at https://doi.org/10.1111/jce.14375