
Introduction: Federally qualified health centers (FQHCs) and health departments (HDs) are essential in providing contraceptive care and ensuring reproductive autonomy for adolescents. Through offering adolescent-specific services and by training providers in adolescent-specific care and patient-centered contraceptive counseling, clinics can ensure access to high quality contraceptive care for adolescents. Despite the significant decrease in adolescent pregnancy rates, rates remain high in the South and in rural counties, suggesting that clinics in these areas may not have the capacity to provide adolescent-specific services and patient-centered counseling. This study compares the capacity to provide adolescent-specific and patient-centered contraceptive services in rural and urban FQHCs and HDs in two southeastern states -- South Carolina (SC) and Alabama (AL).
Methods: Data were collected from a statewide survey of FQHC and HD clinics in SC and AL in 2020. A total of 239 clinics were included (FQHC N=112 and HD N=127) and were identified as rural (N=101) or urban (N=138) using Rural-Urban Continuum Codes. Capacity to provide patient-centered adolescent care is defined as 1) a clinic offering adolescent-specific services; 2) providers at the clinic receiving training in patient-centered counseling; and 3) providers receiving training in adolescent-specific care. To measure capacity, these three survey items were dichotomized into Yes/No responses and then combined into a new variable to measure clinics who responded Yes to each survey item. The type of adolescent-specific services was also measured as being onsite, offsite, outreach, or none. Capacity to provide patient-centered adolescent care was compared across clinics located in rural and urban settings and by clinic type. Statistical differences were determined using the Chi-Square test of independence (α= 0.05).
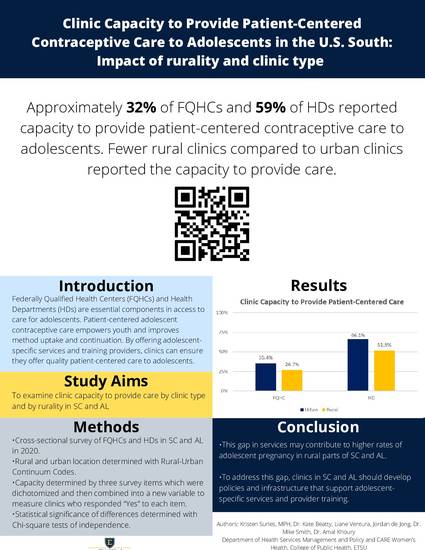
Results: Overall, 44.8% of participating clinics in SC and AL had the capacity to provide patient-centered adolescent contraceptive services. Approximately 51.8% of rural and 66.1% of urban HDs reported the capacity to provide adolescent-specific services. In contrast, 26.7% of rural and 35.4% of urban FQHCs reported the capacity to provide adolescent-specific services. Approximately 55.4% of rural and 71.4% of urban HDs provided any adolescent-specific services, but fewer rural HDs (30.2%) provided onsite services than urban HDs (59.3%) (p=0.003). Fewer than half of rural (42.2%) and urban (48.8%) FQHCs provided adolescent-specific services, with approximately 23.8% of rural and 27.9% of urban sites providing onsite services.
Conclusions: The capacity of clinics in SC and AL to provide contraceptive counseling to adolescents, which is anchored in reproductive autonomy, is contingent upon the provision of adolescent-specific services and provider training. Most clinics, especially rural clinics, did not have the capacity to provide patient-centered contraceptive counseling to adolescents. This gap in services may contribute to the higher adolescent pregnancy rates in rural areas of SC and AL. Clinics in SC and AL, especially FQHCs, should develop policies that support adolescent-specific contraceptive services and provider training.
Available at: http://works.bepress.com/liane-ventura/1/