
- splenic artery pseudoaneurysm; coil embolization; hemorrhagic shock
A 56-year-old Asian male was brought to the emergency department by first responders after he developed severe, sudden-onset headache and chest pain at his home. Past medical history was insignificant. On arrival to the emergency department, the patient was in respiratory distress. Vital signs revealed temperature of 36.0°C, blood pressure of 71/44, heart rate of 90 beats per minute, respiratory rate of 18 breaths per minute, and oxygen saturation of 95% with delivery of oxygen at 2 liters per minute via nasal cannula. Examination of the abdomen revealed diffuse tenderness. Laboratory findings and arterial blood gas analysis revealed normocytic anemia (hemoglobin 7.6 mg/dL) and an anion gap metabolic acidosis with low arterial pH (7.260) and elevated lactic acid (11.0 mg/dL).
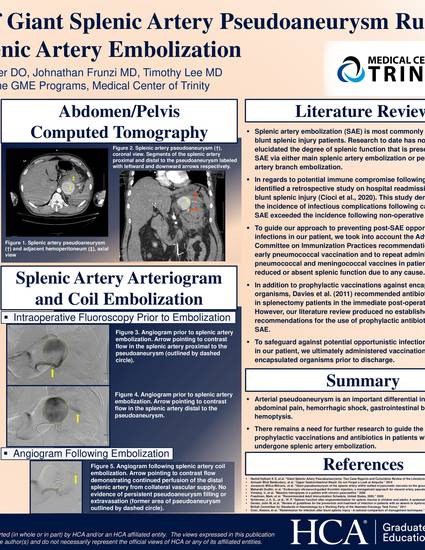
Computed Tomography (CT) of the abdomen and pelvis revealed a splenic artery pseudoaneurysm, with cross-sectional area of 5.8 x 5.6 cm, and intra-abdominal fluid collections consistent with hemoperitoneum. The patient received transfusion of packed red blood cells and resuscitation with intravenous crystalloids. He subsequently underwent selective splenic artery arteriogram and coil embolization with resolution of pseudoaneurysm filling and extravasation. The following day, exploratory laparotomy with hematoma evacuation and intra-abdominal washout was performed. The patient was given the Haemophilus influenzae type B, pneumococcal, and meningococcal vaccines and discharged.
Available at: http://works.bepress.com/johnathan-frunzi/25/