
Introduction: Although, Tele-ICU is integrated into 11% of US critical care delivery, Tele-innovation's advanced monitoring, clinical decision-support functions and cognitive affordances have not been examined in PCU. We compared significant well established outcomes and quality measures between PCU standard of care and PCU Tele-intervention, namely, hospital length of stay (LOS), mortality, APACHE IV severity adjusted mortality and MSDRG severity adjusted mortality.
Methods: Data about n = 13, 421 patients from 6 hospitals (Observational Case Control design) from Jan 2012 – Mar 2015 were analyzed. PCU standard of care control n=7047, PCU Tele-intervention n=6374. PCU inclusion time was defined as PCU Index = first contiguous PCU census encounter > 24 hours (time thresholds derived from greater than median LOS). Intervention group inclusion defined as > 24 hours Tele-intervention during PCU Index time.
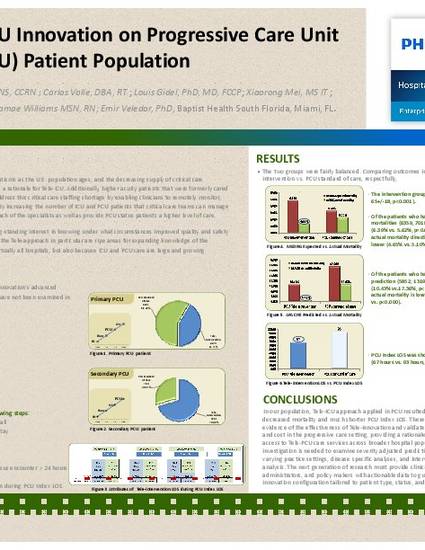
Results:The two groups were fairly balanced. Comparing outcomes in PCU Tele-intervention vs. PCU standard of care, respectfully, the intervention group is older (70+/-16 vs. 65+/-18, p
Conclusions: In our population, Tele-ICU approach resulted in significantly decreased mortality and much shorter PCU Index LOS. These findings provide evidence of the effectiveness of Tele-innovation and validate the impact on quality and cost in the progressive care setting, providing a rationale for extension of access to Tele-PCU care services across broader hospital populations. Further investigation is needed to examine influence of Tele-PCU care service on severity adjusted predictions across varying practice settings.
Available at: http://works.bepress.com/emir-veledar/10/
Winner Clinical Impact Award 2015