
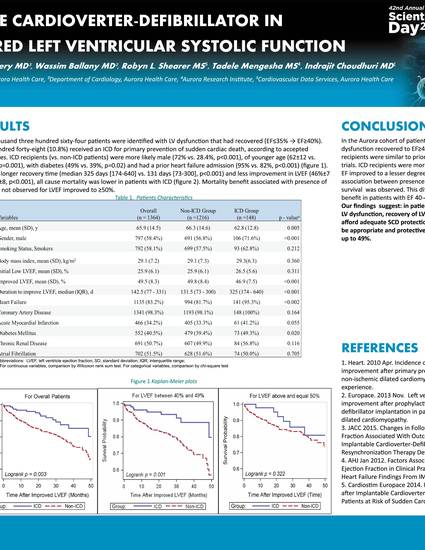
Conclusions: In the Aurora cohort of patients with "transient" LV dysfunction recovered to EF≥40%, characteristics of ICD recipients were similar to prior primary prevention ICD trials. ICD recipients were more likely to have diabetes, and EF improved to a lesser degree and over a longer period. An associated between presence of ICD and better all-cause survival was observed. This difference was driven by a benefit in patients with EF 40-49%.
Our findings suggest: in patients who develop significant LV dysfunction, recovery of LV function to EF>35% does not afford adequate SCD protection, and that ICD therapy may be appropriate and protective in patients with EF improved up to 49%.
Singh K, Zahwe F, Omery B, Ballany W, Shearer R, Mengesha T, Choudhuri I. Benefit of implantable cardioverter-defibrillator in patients with improved left ventricular systolic function. Poster presented at: Aurora Scientific Day; May 25, 2016; Milwaukee, WI.
Aurora Cardiovascular Services, Department of Electrophysiology, Department of Cardiology, Cardiovascular Data Services, Aurora Health Care, Aurora Research Institute